")
")
Paediatric neurosurgery
Alterations in the closure of the cranial sutures (craniostenosis), congenital alterations of the closure of the spinal cord (meningocele, tethered cord etc.), tumors in the central nervous system, cranioencephalic trauma and vascular conditions.

Paediatric neurosurgery is a sub-specialism of neurosurgery dealing with patients under the age of fourteen. Paediatric conditions are different to adult ones both in form and how they are manifested. A child’s brain is not fully formed at the time of birth and keeps developing throughout childhood. Therefore, paediatric conditions are very specialised and should be treated by professionals with experience in treating paediatric patients within a multidisciplinary environment.
Congenital Malformations
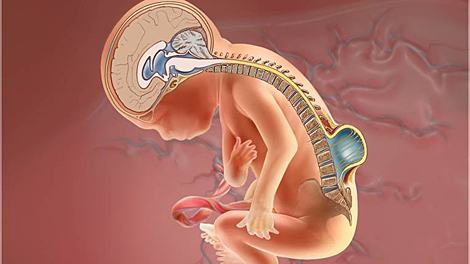
Hydrocephalus: Is the accumulation of excessive cerebrospinal fluid (CSF), which surrounds the brain and medulla spinalis spinal cord. This fluid takes nutrients to the brain, carries away waste from this organ and acts as a shock-absorber. Hydrocephalus means ‘water on the brain’. This accumulation of fluid exerts pressure on the brain and can, if it is not treated properly, lead to neurological problems, damaging or destroying the brain tissue.
In small children, hydrocephalus can be associated with the following conditions:
- Infections in central nervous system (such as meningitis or encephalitis), especially in babies
- Intracerebral haemorrhage during or shortly after birth (especially in premature babies)
- Lesions before, during or after birth, including subarachnoid haemorrhages
- Tumors in the central nervous system, including the brain or medulla spinalis
- Lesion or trauma
- Congenital deformities
The symptoms depend on the cause of the obstruction, the age of the person and the amount of brain tissue damaged through inflammation. In babies with hydrocephalus, the cerebrospinal fluid accumulates in the central nervous system making the fontanelle (the soft spot) protrude so that the head is bigger than expected.
The initial symptoms may also be:
- The eyes seem to face downwards
- Irritability
- Convulsions
- Separated sutures
- Drowsiness
- Vomiting
Other symptoms may be manifested in older children:
- Headache
- Personality changes and memory
- Strabismus or uncontrolled eye movements
- Drowsiness
- Loss of bladder control (urinary incontinence)
- Loss of coordination and problems walking
- Vomit
The diagnosis is given using a clinical examination and symptom analysis and it is confirmed with image tests: an echography for smaller children, or a cranial CT or MRI scan.
The aim of treatment is to minimise or prevent cerebral damage through an improved flow of cerebrospinal fluid (CSF). In a few patients, the hydrocephalus can be controlled through endoscopic procedures (fenestration of the third ventricular floor, aqueductoplasty) or by re-establishing the normal CSF flow (tumour resection, disappearance of intraventricular blood following CTE). However, in most cases, a system to tap the CSF is needed. Given that the great majority of these devices regulate the flow or pressure of CSF using complex control mechanisms, devices are given the name ‘shunts’. The most common ones being VP (ventriculoperitoneal derivation) and VA (ventriculoatrial).
Spina bifida: Is a congenital deformation of the spinal cord which is characterized by the fact that one or vertebral arches did not fuse correctly during the gestation period and the spinal cord is left unprotected by the bones. The main cause of spina bifida is a deficiency of folic acid in the months leading up to the pregnancy and in the following three months, although the cause is unknown in 5% of cases.
Preventing defects in the spinal cord is possible in planned births in the following way:
- Avoid the intake of toxins and teratogenic drugs in the periconceptional period
- Balanced diet
- Intake of folates from the preconception period, at least three months before conception until week twelve of gestation
There are two types of spina bífida, spina bifida occulta and open spina bífida. In spina bifida occulta there is a small defect or opening in one or more vertebrae. Some have a lipoma, dimple, tuft of hair, dark patch or protuberance on the affected region. The spinal cord and the nerves are not affected. Many people with spina bifida don’t know that they have it or the symptoms do not appear until later years.
There are three types of symptoms:
- Neurological: Weakness in the lower limbs, atrophy of a leg or foot, lack of sensitivity or irregular reflexes
- Genitourinary: Urinary incontinence, faeces or urinary retention
- Orthopaedic: Deformity in the feet or difference in size
Open spina bifida - Myelomeningocele: Is a more serious and more common variety. The cyst contains both the membranes and the nerve roots of the actual spinal cord. Sometimes the spinal cord and nerves are not covered. It is necessary to surgically close the opening in the first few hours of life to avoid infection. In general, the higher the affected vertebra or vertebrae, the more serious the consequences
These consequences may include:
- Hydrocephalus: the accumulation of excessive cerebrospinal fluid (CSF) on the brain
- Other neurological disorders normally associated with hydrocephalus:
- Chari malformation: at the caudal part of the cerebellum and sometimes below the foramen magnum
- Syringomyelia: formation or accumulation of CSF in the spinal cord
- Locomotor apparatus disorders:
- Muscular weakness or paralysis, deformities, decrease or loss of sensitivity under the lesion.
- Urinary control issues and intestinal defects which can lead to vesical and/or faecal incontinence or alternatively a retention of one or both types
Urinary infections are common and are caused by a defective bladder; therefore, an intermittent catheter is often used. Treatment for both open and occulta spina bifida requires the surgery to repair the defect in the vertebral duct, its covering and associated malformations thus a multidisciplinary approach is generally required.
Craniofacial Malformations
Craniosynostosis
This condition is common in the first year of life and consists in the premature fusion of the bones of the cranium which can lead to anomalies in the shape of the head with both aesthetic and functional repercussions. One such repercussion is an increase in the intracranial pressure which affects one out of every thousand children, and its treatment requires surgery. The sooner the intervention is carried out, the better the prognosis will be.
Paediatric Neuroncology
Tumours in children are not very common, although the number of cases is increasing. Neuroncology deals with brain tumours, the central nervous system, the spinal cord and peripheral nerves.
This is applied in the following cases:
-
Epilepsy in children: In cases in which the focal seizure is concentrated, it is possible to cure it through surgery. Patients should be examined by a team who can decide what the best treatment for these children is: Only medical or medical and surgical.
- Spasticity: Motor disorders caused by cerebral paralysis or medullary lesions (in adolescents and children). These disorders can be treated by neurotomy or other kinds of surgery designed to improve the patient’s quality of life.




